
By: Natasha Bisarya and Woocheol Kim
This case report describes a 42-year-old male who was referred by an optometrist to our ophthalmologist Dr. Shah with an asymptomatic left inferotemporal cystic lesion with vascular bulbs at the tips, discovered during a routine eye examination. Differential diagnosis includes cavernous hemangioma associated with intracranial vascular anomalies, and retinal astrocytic hamartoma associated with tuberous sclerosis. The importance of ruling out associated intracranial lesions, including vascular malformations and tubers, is emphasized.
Introduction
The patient, a 42-year-old Caucasian male, was referred for a detailed ophthalmological evaluation after a cystic lesion was identified during a routine eye exam. The patient had no complaints of vision loss, floaters, or any other symptoms. There was no significant past medical history and no known family history of eye diseases or systemic conditions like tuberous sclerosis.
Clinical Findings
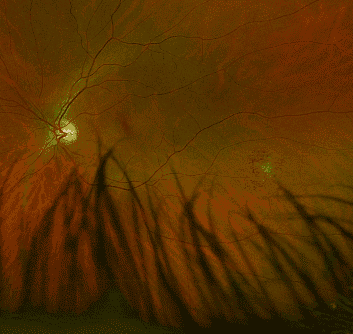
Upon examination, visual acuity was 20/20 in both eyes, and intraocular pressure was within normal limits. Slit-lamp examination was unremarkable in both eyes. Dilated fundus examination revealed a lesion in the inferotemporal region of the left eye. The lesion appeared cystic, with distinct vascular bulbs at the tips. No other abnormalities were noted in either eye.
Diagnostic Tests
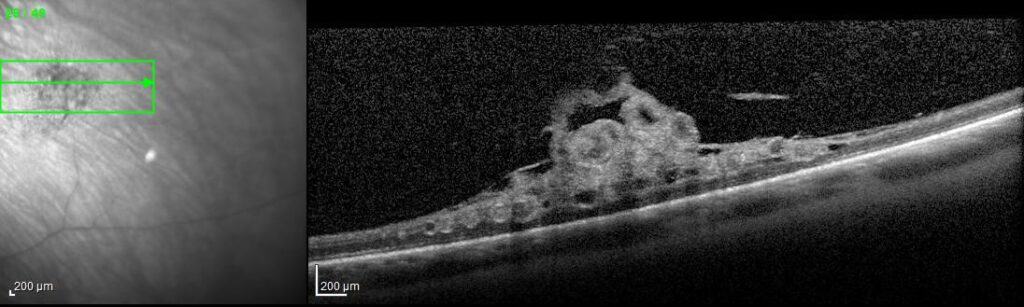
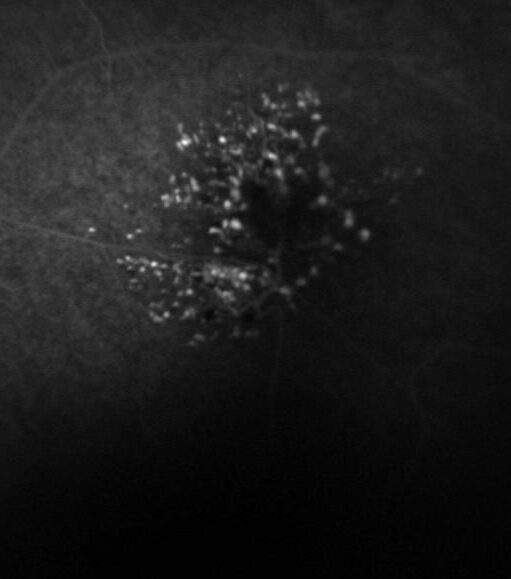
OCT (Optical Coherence Tomography) confirmed the central cystic nature of the lesion with surrounding retinal tissue appearing structurally normal. Fluorescein angiography showed hyperfluorescence with late staining, but no leakage. MRI of the orbit and brain was recommended to rule out intracranial involvement.
Differential Diagnosis
- Cavernous Hemangioma associated with Intracranial Vascular Anomalies: The cystic nature of the lesion with vascular bulbs may be indicative of a cavernous hemangioma. These are known to occur sporadically but may also be associated with intracranial vascular malformations.
- Retinal Astrocytic Hamartoma associated with Tuberous Sclerosis: Given the patient’s age and the appearance of the lesion, retinal astrocytic hamartoma was also considered. These benign lesions are often associated with tuberous sclerosis and can have similar clinical features.
- Retinal Vaso-proliferative tumors associated with sub-retinal exudation and potential subretinal fibrosis. These tumors can be distinguished from Cavernous Hemangioma by the absence of vascular bulbs, and from Retinal Astrocytic Hamartoma by not showing the characteristic calcified retinal nodules associated with Tuberous Sclerosis.
Importance of Ruling out Intracranial Lesions
The presence of either a cavernous hemangioma or an astrocytic hamartoma raises the suspicion for associated intracranial lesions such as vascular malformations in the former and tubers in the latter. Failure to identify these intracranial anomalies may lead to severe neurologic consequences, including seizures, hemorrhages, or more serious complications.
Management and Follow-up
Given the uncertainty of the diagnosis, the patient was referred for an MRI of the orbit and brain, and consultation with a neurologist was recommended for further evaluation of potential intracranial lesions. Genetic testing for markers of tuberous sclerosis was also advised.
Conclusion
This case emphasizes the significance of comprehensive evaluation for patients presenting with retinal lesions. A multidisciplinary approach involving retina specialists, other eye doctors, and neurologists. This can be crucial for accurate diagnosis and management, especially in cases where intracranial involvement is suspected.
References
- Shields JA, Shields CL. Atlas of Intraocular Tumors. Lippincott Williams & Wilkins; 1999.
- Osborne, A.G., Blaser, S.I., Salzman, K.L. et al. Diagnostic Imaging (7th ed.). Elsevier; 2020.
- Roach ES, Gomez MR, Northrup H. Tuberous sclerosis complex consensus conference: revised clinical diagnostic criteria. J Child Neurol. 1998;13(12):624-628.